Dear All:
I wrote twice last week with materials from the 5-8 Sep ASM-ESCMID conference (EMA-FDA-NICE updates and the CARB-X + GARDP Bootcamps. But there’s more … in parallel, we last week also had the final DRIVE-AB conference in Brussels! In the absence of a Star Trek transporter it was not possible to attend both, but I did hear from others who attended and I also gave a talk at the ASM-ESCMID conference in which I summarized some of the material from the final DRIVE-AB conference.
My summary talk can be downloaded here. Highlights for your consideration would be:
- Antibiotics are the fire extinguishers of medicine, but we currently pay for them as if we were paying the fire department on a per fire basis. As you know well, this is the fundamental economic hurdle to overcome.
- As a path to transforming the way policymakers stimulate innovation, responsible use and global access to novel antibiotics to meet public health needs, DRIVE-AB sought solutions that were consistent with the principles of Access, Sustainable Use, and Innovation.
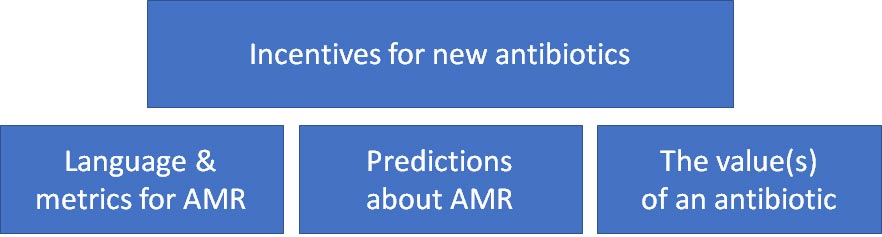
- To achieve this, DRIVE-AB created 4 blocks of insight: (1) a common language for measuring things like sustainable use, (2) models to predict emergence & spread of AMR, (3) new HTA metrics for antibiotic value, and (4) incentive models.
- The first three of these elements are the building blocks that support the fourth element, the incentive models for antibacterial R&D (see graphic below).
- Four incentive models are recommended. Two provide Push (Grants & a Pipeline Coordinator) and two provide Pull (Market Entry Rewards and a Long-Term Continuity Model). All four of these models are important as they together drive innovation, while supporting sustainable use and access. Push incentives alone are not sufficient
- Note that there is pop-quiz buried in the slide deck. The answer is found at the very end of this email … try not to look too soon!
More details + a variety of official written reports will be forthcoming from DRIVE-AB over the next few months. And of course we now have to take the big step of making a Market Entry Reward (or two or three) happen. There is nothing definitive yet in any territory, but I am aware of a number of discussions that are making strong headway. It won’t be easy, but DRIVE-AB has definitely achieved its goal of creating the required mutual understanding among a wide group of stakeholders with diverse backgrounds.
And while DRIVE-AB has been the work of many hands, I want to in particular call out the contributions of 4 individuals. First, Stephan Harbarth (University of Geneva) and Judy Hackett (AstraZeneca) did a splendid job as the academic and industry co-leads for the overall project. And Christine Årdal (Norwegian Institute of Public Health) and David Findlay (GSK) demonstrated true leadership skills as they crystallized and summarized the debates around the incentive models.
Having been there at the birth of DRIVE-AB (James Anderson of GSK and I spent many hours working with EFPIA’s Richard Bergstrom and Brendan Barnes on the basic design of the project), I am just delighted to see it all coming to fruition! I know that it times it felt like (and was like) herding cats but we all owe these four a debt of thanks for their many hours of effort.
All best wishes, –jr
John H. Rex, MD | Chief Medical Officer, F2G Ltd. | Chief Strategy Officer, CARB-X | Expert-in-Residence, Wellcome Trust. Follow me on Twitter: @JohnRex_NewAbx. See past newsletters and subscribe for the future: https://13.43.35.2/blog/
Upcoming meetings of interest to the AMR community:
- 13 Sep 2017 (DC): FDA-CDRH workshop on diagnostic devices for detecting antimicrobial susceptibility & resistance
- [NEW] 1 Oct 2017 (London): BSAC: AMR Market Lounges. Networking day.
- 4-8 Oct 2017 (San Diego): IDWeek
- [NEW] 10 Oct 2017 (Hanoi): UK-Vietnam Newton Fund Pre-Call Workshop on Partnership for Infectious Disease Research 2017.
- 29 Oct-1 Nov 2017 (Santa Fe): Keystone Symposium – Antimicrobials and Resistance: Opportunities and Challenges
- [NEW] 2 Nov 2017 (London): BSAC: AMR Market Lounges. Networking day.
- 11-19 Nov 2017 (Annecy, France): International Course on Antibiotics and Resistance (ICARE)
- [NEW] 20 Nov 2017 (week of, China): UK-China Newton Fund Workshop: Antimicrobial Resistance Centre Partnerships Initiative.
- [NEW] 20 Nov 2017 (London): Early Career Researcher Workshop on Diagnostics for Antimicrobial Resistance.
- 24-27 Nov 2017 (Taipei): 30th International Congress of Chemotherapy & Infection (ICC)
- 12-14 Feb 2018 (Baltimore): ASM Biothreats Conference
- 11-16 Mar 2018 (Ventura Beach): Gordon Research Conference on Antibacterial Discovery
- 21-24 Apr 2018 (Madrid): ECCMID
- 7-11 Jun 2018 (Atlanta): ASM Microbe
- 22-27 Jul 2018 (Bryant University, Smithfield, RI): Gordon Research Conference on Drug Resistance for Cancer, Infectious Disease and Agriculture
PS: The answer to the pop quiz is that a reasonable rule-of-thumb would be $20m/year.